
Written Statement for the Record
Of
The National Association of ACOs
For the
Senate Committee on Finance
Hearing on
“Bolstering Chronic Care through Medicare Physician Payment”
April 11, 2024
The National Association of ACOs (NAACOS) appreciates the opportunity to submit a statement to the Senate Committee on Finance in response to the hearing “Bolstering Chronic Care through Medicare Physician Payment.” NAACOS represents more than 430 accountable care organizations (ACOs) in Medicare, Medicaid, and commercial insurance working on behalf of health systems and physician provider organizations across the nation to improve quality of care for patients and reduce health care cost. NAACOS members serve over 9 million beneficiaries in Medicare value-based payment models, including the Medicare Shared Savings Program (MSSP) and the ACO Realizing Equity, Access, and Community Health (REACH) Model, among other alternative payment models (APMs). NAACOS appreciates the committee’s leadership and commitment towards improving the Medicare payment system. Our statement reflects the shared goal of our members to advance value-based care.
APMS ARE A PLATFORM FOR IMPROVING CHRONIC CARE MANAGEMENT
A key aim of health care should be keeping patients healthy and supporting them with getting the right services, at the right time, in the right place. Unfortunately, Medicare’s fee-for-service (FFS) payment system can lead to care fragmentation that results in reactive, sickness-based care. This means higher costs and less coordinated care for patients. The current physician payment system also underinvests in primary care and care coordination and does not account for adequately paying providers as costs rise. As a result, physician practices have limited funding or tools to proactively manage complex patient care. Stabilizing Medicare’s payment system and ensuring payment adequacy along with strong incentives to adopt infrastructure and staffing necessary for population health is needed to transition into payment models that focus on outcomes.
APMs have proved to be the solution. Over the last two decades, the growth of APMs has enabled health care providers to work as a team and make necessary investments that result in better outcomes and reduced costs. APMs are becoming more rooted in our health care system but growth has been slower than Congress’ original goal. It is essential to remove barriers to participation and give additional flexibility and tools to innovate care.
ACOs are the Largest APM Leading Medicare’s Value Transformation
The MSSP is the largest and most successful value-based care program in Medicare, and as such it should be utilized as an innovation platform. In 2024, there are 602 ACOs coordinating care for 13.4 million Medicare beneficiaries. ACOs are a voluntary alternative to the fragmented FFS system that gives doctors, hospitals, and other health care providers the flexibility to innovate care and holds them accountable for the clinical outcomes and cost of treating an entire population of patients.
With primary care as the backbone, ACOs employ a team-based approach that allows clinicians to ensure patients receive high quality care in the right setting at the right time. ACOs improve quality while controlling costs through primary care-focused initiatives such as expanded primary care teams, care coordination strategies, and enhanced data and analytics tools for primary care practices.[1] The ACO model also provides an opportunity for providers to work collaboratively along the continuum while remaining independent.
Importantly, ACOs provide shared savings opportunities and enhanced regulatory flexibility that allows clinicians to maintain financial security while practicing medicine more freely. For example, many primary care practices were financially harmed by the effects of the COVID-19 pandemic, and evidence showed that independent primary care practices participating in ACOs were better-equipped to respond to the crisis, supported by alternative revenue sources and workflow tools made available through ACO participation.
It’s clear these payment system reforms have been a good financial investment for the government. In the last decade, ACOs have generated more than $22.4 billion in savings with $8.8 billion being returned to the Medicare Trust Fund while maintaining high quality scores for their patients. The growth of APMs has also produced a “spill-over” effect on care delivery across the nation, slowing the overall rate of growth of health care spending. Providers in APMs also help make the Medicare program stronger by reducing improper payments. Using enhanced data and analytics, ACOs regularly identify and report instances of fraud, waste, and abuse.
Develop Solutions to Improve Physician Payment and Encourage the Movement to Value
The Medicare Access and CHIP Reauthorization Act (MACRA) included advanced APM incentive payments to encourage providers to move into risk-based payment models while also providing funds that allow them to cover services not reimbursed by traditional Medicare (e.g., meals programs and transportation). These are the types of services that help address patients’ social needs, keep patients healthier, and lower costs. MACRA also included a higher conversion factor update for clinicians in advanced APMs, however this does not adequately address inflation, creates more complexity for clinicians, and could make it harder for clinicians in APMs to successfully meet program financial targets.
While NAACOS is pleased that Congress passed another short-term extension of MACRA’s advanced APM incentives, it does not go far enough to drive long-term movement to value-based care. The next year when financial incentives favor clinicians that participate in risk based APMs, over those who remain in FFS, will be 2032 (see graph below).
For clinicians in advanced APMs, the 1.88 percent incentive for 2024 and higher conversion factor is a lower incentive than the maximum Merit-Based Incentive Payment System (MIPS) adjustment, which is estimated to be just over 3 percent. As the incentive structure shifts, some clinicians may choose to voluntarily shift back to MIPS because the program will continue to offer opportunities for high performing clinicians in APMs to qualify for higher financial incentives.

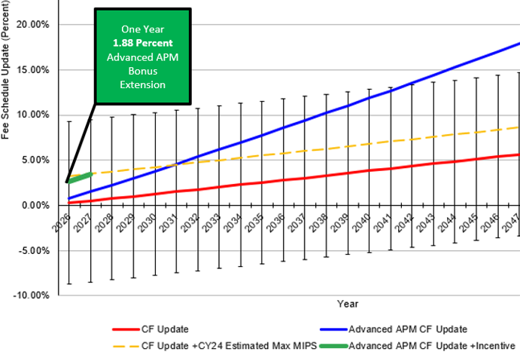
- In 2026, clinicians in MIPS will be provided a 0.25 percent conversion factor update (red line) and can receive an additional positive payment adjustment in MIPS.
- While the maximum potential incentives under MIPS are 9 percent, CMS estimates that the highest MIPS adjustments will be around 3 percent in the coming years.
- Accordingly, the total potential payment adjustment is an estimated 3.25 percent (yellow dashed line).
- Conversely, clinicians in advanced APMs will only receive a 0.75 percent conversion factor update (blue line) and be eligible for a 1.88 percent incentive payment, a total incentive equal to 2.63 percent (Green line).
The 1.88 percent advanced APM incentive will also expire at the end of 2024. The expiration of APM incentives will mean a significant incentive shift towards MIPS in the short-term. APM adoption has been steadily growing but still falls below Congress’ original goals of transitioning all clinicians into models with financial risk.
Going forward the committee should:
- Develop approaches that account for inflation in payment updates.
- Maintain stronger financial incentives for physicians that move into APMs.
- Ensure that incentives do not impact a clinician’s ability to meet financial targets in APMs.
Reduce Program Complexity & Improve Scaling of Innovation
MACRA created nonfinancial incentives for clinicians in APMs by exempting them from regulatory burdens associated with the FFS payment system. Unfortunately, program complexity can lead to less participation in value models. Additionally, clinicians can be hesitant to participate in Innovation Center model tests because the models do not have a predictable pathway to permanence.
Going forward the committee should:
- Reduce program complexity by ensuring that clinicians in APMs are not required to engage in duplicative quality reporting efforts.
- Emphasize that MIPS should prepare clinicians for and encourage adoption of APMs.
- Ensure that promising aspects of innovative models have a more predictable pathway for becoming permanent.
While updating Medicare’s payment system and incentive structure will take time, in the short term, the committee should advance the Value in Health Care Act (H.R. 5013/S. 3503). This bipartisan bill was introduced by Senators Sheldon Whitehouse (D-RI), John Barrasso, M.D. (R-WY), Peter Welch (D-VT), Thom Tillis (R-NC), Bill Cassidy, M.D. (R-LA), John Thune (R-SD), and Marsha Blackburn (R-TN). It makes several important reforms to ensure that APMs continue to provide high-quality care for Medicare beneficiaries, including:
- Providing a multi-year commitment to reforming care delivery by extending MACRA’s original 5 percent advanced APM incentive for two years to continue to encourage the movement to value.
- Ensuring that qualifying thresholds remain attainable to promote program growth by freezing them at 50 percent for two years and giving the Centers for Medicare & Medicaid Services (CMS) authority to adjust thresholds through rulemaking and set varying thresholds for more targeted models where participants (e.g., specialists) cannot meet the existing one-size-fits-all thresholds.
- Removing the revenue-based designation in MSSP that penalizes certain ACOs, especially those including rural and safety net providers.
- Establishing guardrails for CMS to ensure that the process to set financial benchmarks is transparent and appropriately accounts for regional variations in spending, to prevent arbitrary winners and losers.
- Directing CMS to establish a voluntary, full-risk track within programs like the MSSP and has the U.S. Department of Health and Human Services provide more technical assistance to new APM participants.
- Directing the Government Accountability Office to evaluate the potential of parity between APMs and Medicare Advantage (MA), so policymakers can seek greater alignment between the programs to ensure that both models provide attractive, sustainable options for innovating care delivery, and to ensure that APMs do not face a competitive disadvantage.
Build on the Innovation Center’s Successes
As the Center for Medicare and Medicaid Innovation (CMMI) tests new payment models, successful models, or key aspects of those models, should be embedded as permanent parts of Medicare via the MSSP. While the MSSP currently includes various participation options with increasing levels of risk and reward, there is currently no full-risk option for ACOs participating in MSSP. Congress should direct CMS to create a separate full-risk option within MSSP to serve as a better bridge between it and ACO REACH. This “Enhanced Plus” Track should include greater flexibility in payment design and available waivers. As the only permanent total cost of care model in Medicare, the MSSP should be adapted to remain a viable option for more advanced ACOs and further advance value-based care.
Population-Based Payments for Primary Care
More flexible payment mechanisms can support care delivery transformation, strengthen primary care, and increase participation in ACO initiatives. CMS recently launched the ACO Primary Care Flex model, which will allow MSSP ACOs to offer prospective population-based payments for primary care. NAACOS has been advocating for this approach, which will bolster primary care practices in ACOs. Shifting to prospective payments provides primary care practices with stable and predictable cash flow needed to transform care delivery and provide comprehensive, team-based care. For more than a decade, the ACO model has improved beneficiary outcomes, generated savings to Medicare and allowed practices to invest shared savings into innovation and patient care. This model builds on the success of MSSP while recognizing we must continue to evolve the program for growth to continue.
While we are extremely pleased with the model, we are concerned that excluding high-revenue ACOs will prevent many independent primary care practices who have partnered with their local health systems from taking advantage of these much-needed innovations. The premise of ACOs is to bring together providers from across the continuum of care to provide improved care for beneficiaries. This is a primary example of why the committee should support removing the revenue-based designation in MSSP that continues to penalize certain ACOs.
Expand Waivers for APMs
Current law allows CMS to waive certain Medicare FFS requirements in MSSP and other APMs. This is a critical component of APMs as it allows providers to operate with fewer restrictions leading to a reduction in provider burden and increased care innovation. However, the waivers to date have been limited and can also be burdensome for providers. For example, MSSP only has waivers for telehealth and the 3-day rule for skilled nursing facility stays. Yet the ACO REACH model has access to many more waivers. We believe all APMs should have access to all available waivers and that those waivers shouldn’t be limited to certain models. Congress should direct CMS to establish a common set of waivers for APMs.
Chronic care management (CCM) is also a critical part of coordinated care. Unfortunately, Medicare’s current CMM codes include a beneficiary cost-sharing obligation that creates barriers to care. While APMs offer opportunity to allow providers to reduce beneficiary cost sharing to ensure patients receive enhanced care management, we encourage the committee to look at legislative options to waive the beneficiary coinsurance related to CCM. This would help ensure that more chronically ill Medicare patients can receive access to high-quality care.
Improve Approaches to Test and Scale Innovation
While CMMI has been successful in testing innovative payment arrangements and increasing adoption of APMs, the success of these models is not captured within current evaluation approaches. Congress should work with CMS to ensure that promising models have a more predictable pathway for being implemented and becoming permanent and are not cut short due to overly stringent criteria. This includes broadening the criteria by which CMMI models qualify for Phase 2 expansion and directing CMMI to engage stakeholder perspectives during APM development.
Establish Parity Between APMs and Medicare Advantage Program Requirements
Recognizing ACOs’ and MA’s shared goals of improving the quality of care and cost savings to patients, it’s imperative to build parity between the two programs. Misaligned incentives are harmful to advancing value as they increase provider burden, create confusion and disincentives for patients, and generate market distortions that favor one entity over another. Parity can be better provided in the programs’ benchmark and risk adjustment policies, quality measurement, and marketing requirements. ACOs should be allowed to provide comparable benefits to those offered to MA patients, such as telehealth visits, transportation benefits, home visits, etc. Without parity, providers are forced to spend time managing the various program requirements rather than managing patient care. Congress should direct GAO to evaluate how to create more parity between APMs and MA. Additionally, Congress should explore opportunities to incentivize MA plans to enter risk-bearing arrangements with providers.
We thank the committee for this opportunity to provide feedback on this important hearing. NAACOS and its members are committed to providing the highest quality care for patients while advancing population health goals for the communities they serve. We look forward to our continued engagement on bolstering CCM through payment system reforms. If you have any questions, please contact Aisha Pittman, senior vice president, government affairs at aisha_pittman@naacos.com
